Family Planning in Humanitarian Settings: A Strategic Planning Guide
In tribute to the work and life of Jennifer Schlecht, “Women who are displaced have the same reproductive health needs as other women — if not more. I think there is an increased acceptance and understanding that crises are not something that happens to other people. [This understanding] opens so many more opportunities for all of us.”

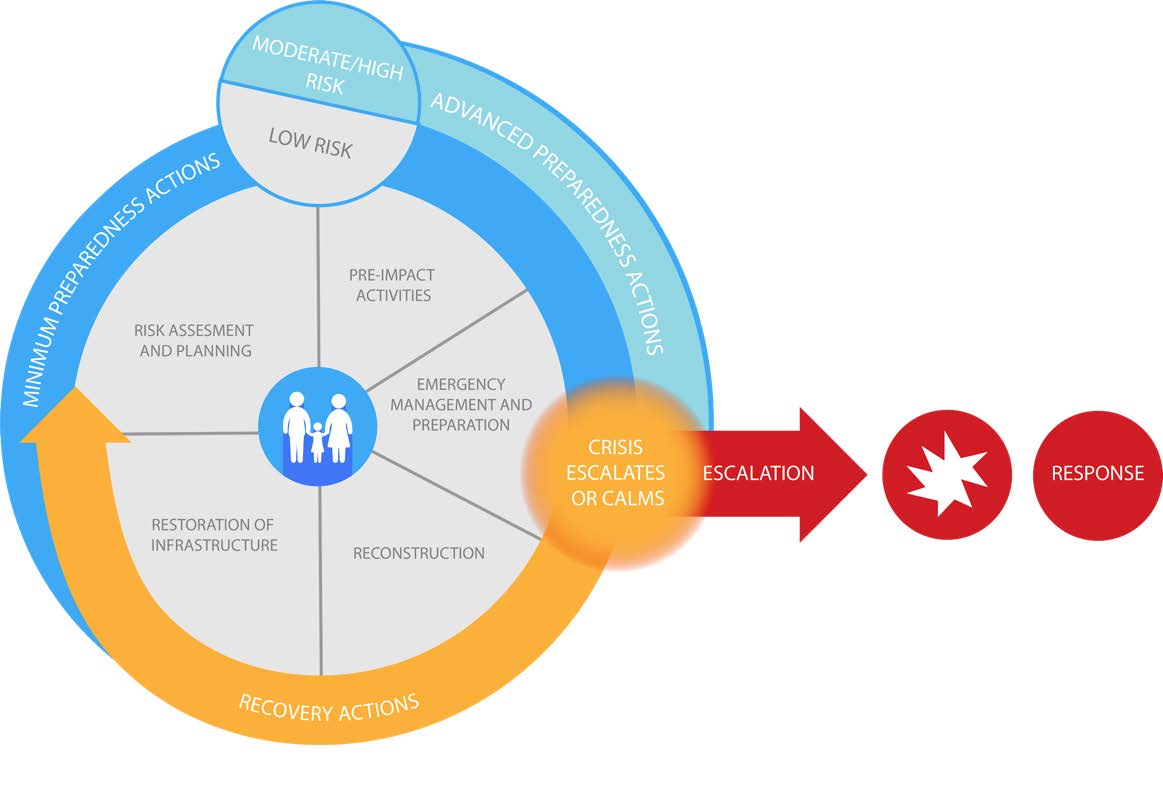
The Humanitarian Cycle highlights the three main overlapping phases in a humanitarian crisis: preparedness, emergency response, and recovery.
Family planning is lifesaving.1 Ensuring continuous access to family planning for populations experiencing a humanitarian crisis is needed, demanded and feasible. Disruption in family planning services can be minimized through a) preparedness actions, b) crisis response, and c) coordinated transition back to routine services.
The updated Minimum Initial Service Package (MISP)i for Reproductive Health (2018) repositioned family planning “preventing unintended pregnancies”— as one of four main clinical and lifesaving services of the MISP.2
This document leads national and sub-national decision-makers through a strategic process to identify actions that improve family planning access in places at risk of, experiencing, and recovering from crisis events. Actions put forward here represent learning across countries and agencies that have engaged in emergency preparedness, response and recovery, and are informed by experts who have worked across these phases of crisis.ii
There are three main overlapping phases in a humanitarian crisis — preparedness, emergency response, and recovery (see illustration). These phases are often broken down further and do not have clearly delineated start and end points. Countries may be in a prolonged crisis response while preparing for, transitioning from, or experiencing other simultaneous crises. Preparedness, response and recovery efforts should be tailored to local contexts and shaped by decision makers at appropriate points within the humanitarian cycle and within the health system. The Humanitarian Cycle (illustration) highlights these entry points: preparedness, response, and recovery. Stakeholders vary depending on the phase and severity of crisis, and the capacity of international, national and sub-national structures.
Preparedness Actions
Preparedness actions improve the timeliness and quality of a response and increase efficiency during a crisis event.3 Governments that invest in conducting preparedness activities can realize significant cost-savings — reducing the overall strain on over-burdened local and international humanitarian systems and helping to ensure that development gains are not lost when crisis strikes.
Action 1: Review and update policies, strategies and laws to facilitate access and minimize disruption to voluntary family planning services during a crisis event
- Identify opportunities to engage humanitarian actors in technical working groups, such as those working on commodity security or family planning/reproductive health during stable times.
- Advocate for inclusion of family planning/reproductive health within National Emergency and Disaster Risk Management plans.
- Ensure that family planning commodities are included in national essential medicine lists.
- Identify and build capacity for emergency Health Information System if existing system fails.
Action 2: Position current work force and engage non-traditional actors capable of facilitating access to voluntary family planning services during a crisis prior to an emergency
- Train relevant staff at all levels of the health system on the MISP, the Inter-Agency Emergency Reproductive Health Kitsiii that facilitate implementation of the MISP, and emergency coordination systems.
- During stable times, engage local actors with the capacity to provide essential family planning/reproductive health services during a crisis event (such as organizations experienced in humanitarian response, private or non-governmental organizations experienced with serving vulnerable populations, groups working in gender-based violence, etc.).
- Involve communities in regions at higher risk of experiencing a crisis in planning and priority setting activities.
Action 3: Prepare family planning/reproductive health supply chains for emergencies including developing risk management capacity, contingency planning, and emergency commodity procurement plans
- Create an enabling policy environment to facilitate rapid entry of family planning commodities into a country in the event of an emergency.
- Map out likely needs, challenges, and contingencies along the supply chain.
- Strengthen national human resource capacity to manage contraceptive supplies in the event of an emergency.
- Integrate emergency supplies (including contraceptives) into logistics management information systems.
- Improve coordination mechanisms across partners to improve supply chain functioning in emergencies.
- Decentralize stock regionally or pre-position key supplies when strategic.
Action 4: Prepare staff and health facilities to mobilize during a crisis event
- Crisis events frequently occur in communities with weak infrastructure and systems. Therefore, strengthening routine services, particularly in high-risk communities, is an important step in preparedness.
- Create a roster of family planning providers, for surge capacity
- Support policies and practices to maximize access to and quality of family planning services, including in crisis situations.
- Task shifting/sharing policies and practice
- Community health workers
- Mobile outreach service delivery
- Disseminate information using a variety of communications channels, e.g., mass media, community group engagement, digital platforms
Crisis Response
Crisis response activates the humanitarian cluster system, including a health cluster and sexual and reproductive health sub-cluster, to ensure coordination within each sector across both existing partners and new partners that enter to provide relief. The reproductive health crisis response, including family planning, is organized around the MISP, as mentioned above.
Action 1: Ensure provision and tracking of voluntary family planning services within a broader health response
- Advocate for the inclusion of the full range of contraceptive methods in the crisis response.
- Advocate to waive policies that block access to family planning services (e.g. residency requirements, eligible couple registration, etc.).
- Monitor implementation of voluntary family planning services within the crisis response.
- Coordinate with other clusters as needed, such as the Logistics Cluster to facilitate availability of family planning supplies.
- Establish interim guidance to support potentially transient populations, such as extending the number of months of oral contraceptive pills provided, distribution of prophylactic emergency contraception, information on the management of longer-term methods, etc.
- Support community engagement that sensitizes communities to the importance of family planning and availability of contraception.
- Support social accountability, including a transparent cycle for reviewing and responding to feedback at the service delivery and cluster coordination level.
Action 2: Leverage routine systems to ensure efficient use of resources
- Review family planning provider roster for recruitment into response team.
- Adapt national Health Information System to collect data from new family planning service delivery points.
- Incorporate changes in contraceptive use and adapt quantification and procurement plans before emergency services end.
Coordinated Transition
Coordinated transition to routine family planning systems should be an early consideration. Such transitions should occur as soon as possible and often can begin three to six months after a crisis event occurs. The transition should be done with minimal disruption to service delivery.
Action 1: Support government to re-establish routine family planning services in crisis-affected areas
- The Ministry of Health should oversee transition from crisis response to routine services.
- Family planning/reproductive health humanitarian actors responsible for interim programming should provide information to the Ministry and development partners including services provided, capacity improved, systems utilized and recommendations for continuity.
- Establish a transition plan for service delivery, human resources, and commodities and supplies, including referral plans to ensure that clients served by interim service delivery points know where to access services.
Action 2: Restore routine family planning supply chains and reduce reliance on humanitarian kits and supplies
- Calculate family planning commodity needs and costs as the situation stabilizes, to inform planning for routine supply chains.
- Include newly introduced family planning commodities within regular supply chain.
- Restore pre-disaster National Supply Chain management mechanisms, in settings where humanitarian actors had taken on those responsibilities.
Action 3: Prepare the health workforce to meet the long-term family planning needs of crisis-affected people
- Train and support providers to understand and respond to the impact of the crises on clients (e.g., psychosocial and physical trauma, increase in adolescent pregnancy, increases in all forms of gender-based violence).
- Ensure the workforce is trained in new or adapted procedures, such as those required to offer new methods introduced during the crisis.
Action 4: Re-establish national information systems for monitoring and tracking family planning services and supplies in crisis-affected areas
- Restore pre-crisis national health management information systems and LMIS and ensure the transfer of data from information systems used during the emergency.
Action 5: Mobilize resources to strengthen the delivery of routine family planning services in crisis-affected areas and beyond
- Leverage new opportunities and partners to improve services following the crisis, such as mobile outreach service delivery.
- Ensure family planning services and supplies are adequately budgeted in post-crisis health and recovery plans.
References
- Winikoff, B., & Sullivan, M. (1987). Assessing the Role of Family Planning in Reducing Maternal Mortality. Studies in Family Planning, 18(3), 128; Ahmed, S., Li, Q., Liu, L., & Tsui, A. O. (2012). Maternal deaths averted by contraceptive use: an analysis of 172 countries. The Lancet, 380(9837), 111–125.
- Inter-Agency Working Group on Reproductive Health in Crisis. (2019) Minimum Initial Service Package for Sexual and Reproductive Health. https://iawg.net/resources/misp-reference
- UNICEF/World Food Programme Return on Investment for Emergency Preparedness Study (2015).
https://www.wfp.org/publications/unicefwfp-return-investment-emergency-preparedness-study
Suggested Citation
High-Impact Practices in Family Planning (HIPs). Family Planning in Humanitarian Settings: A Strategic Planning Guide. Washington, DC: Family Planning 2020, 2020 Sep. Available from: https://fphighimpactpractices.org/guides/family-planning-in-humanitarian-settings/
For more information on HIPs briefs and on the work of the HIPs partnership, please refer to the High Impact Practices in Family Planning website at www.fphighimpactpractices.org or contact the team at http://fphighimpactpractices.org/contact/.
i The set of priority objectives, including access to contraception, and activities to meet basic RH needs in crisis.
ii This document was written by Jennifer Schlecht with critical review and input from Raya Alchukr, Sara Casey, Nadine Cornier, Henia Dakkak, Meghan Gallagher, Stephanie Gee, Aditi Gosh, Jennie Greaney, Nancy Harris, Anushka Kalyanpur, Rajat Khosla, Yann Lacayo, Kathleen Myer, Elizabeth Noznesky, Sarah Rich, and Ashley Wolfington.
iii Standardized reproductive health kits are designed to respond to various population sizes and needs. Family planning kits contain condoms, oral and injectable contraceptives, and intrauterine devices.